
Proven outcomes.¹,²,³
Superior value.¹,³
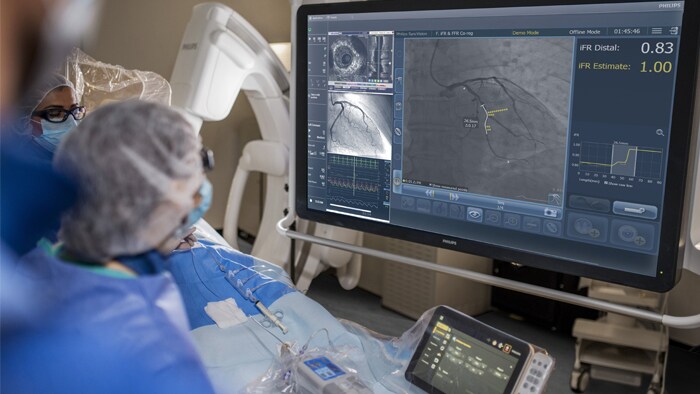
iFRは、診断およびインターベンション処置の内圧計測において、血管拡張剤を必要としないPhysiology指標です。フィリップスのみが提供する
iFRのコレジストレーションは、Physiology計測値を血管造影図に直接マッピングし、PCIの治療戦略を立てるうえでの補助的役割を担います。
主要ガイドラインに掲載された iFR
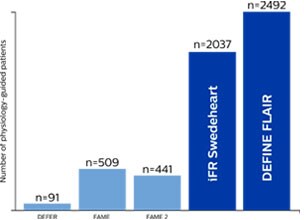
過去最大規模のPhysiology試験において患者転帰データが検証されている iFR
実証された結果
卓越した価値
実証された結果
卓越した価値
治療すべき場所を把握する方法
")
DEFINE PCI
隠れた局所性病変により残存虚血が発生¹⁰

iFRではLADのDeferralがより安全⁹
DEFINE PCI
隠れた局所性病変により残存虚血が発生¹⁰
iFRではLADのDeferralがより安全⁹
ポッドキャストを聴く
Physiology評価の役割
Nick Curzen教授とRasha Al-Lamee博士による、複雑なPCIにおけるPhysiology評価の役割についての議論をお聴きください。 主な論点は次のとおりです。

IntraSight の紹介
スマート、シンプル、シームレス。
新しいPhilips IntraSightインターベンションアプリケーションプラットフォームは、最適な患者ケアを支援する画像撮影、生理学、コレジストレーション¹¹、ソフトウェアを統合します。IntraSightは、iFR/FFR、IVUS、コレジストレーション¹¹などの臨床的に実証された一連の包括的なモダリティを提供して、複雑なインターベンションを簡素化し、ルーチン的な処置のスピードを向上させ、患者ケアを改善します。
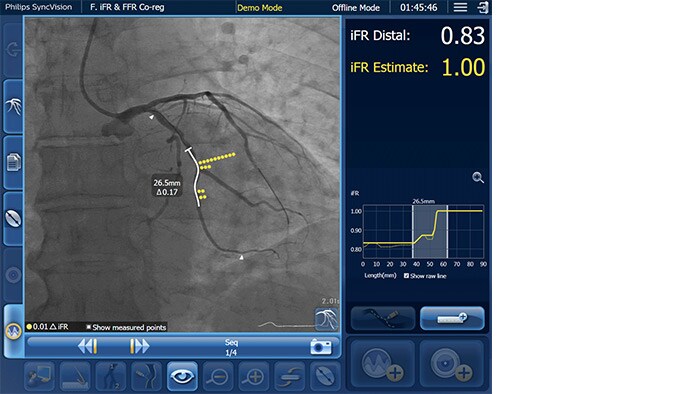
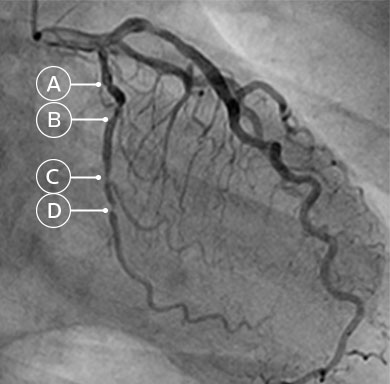
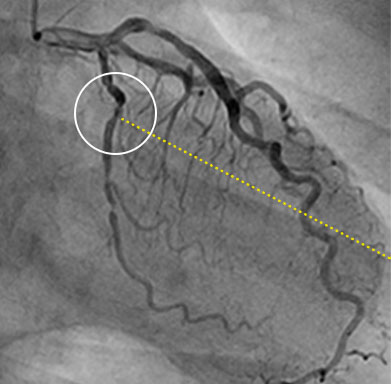
iFR の値を血管造影図に直接マッピングできるため、血管のどの部分が虚血を起こしているのか、正確に見ることができます
新しいPhilips IntraSightインターベンションアプリケーションプラットフォーム上で、Coreシステムのアップグレードとして使用可能。
iFR コレジストレーションを使用すべき理由
iFR コレジストレーションによるPCIの至適化
iFR コレジストレーションを使用して疾患の位置を特定し、ステント前にPCIの影響を想定する方法について、Justin Davies博士が説明します。

iFR コレジストレーションによる
PCI実施方法の変革
PCIを計画する際には、虚血があるかどうかだけでなく、どこにあるかを理解する必要があることを、Allen Jeremias博士が説明します。
DEFINE PCIの結果
4名のうち1名の患者が、PCI後に残存虚血を抱えたままカテーテル検査室を後にします。その多くは隠れた局所性病変によるものです。¹⁰
iFR コレジストレーションを使用すべき理由
iFR コレジストレーションによるPCIの至適化
iFR コレジストレーションを使用して疾患の位置を特定し、ステント前にPCIの影響を想定する方法について、Justin Davies博士が説明します。
iFR コレジストレーションによるPCI実施方法の変革
PCIを計画する際には、虚血があるかどうかだけでなく、どこにあるかを理解する必要があることを、Allen Jeremias博士が説明します。
DEFINE PCIの結果
4名のうち1名の患者が、PCI後に残存虚血を抱えたままカテーテル検査室を後にします。その多くは隠れた局所性病変によるものです。¹⁰

DEFINE PCIの主要な知見に関する専門家の議論
Allen Jeremias博士、Gregg Stone博士、Habib Samady博士、Manesh Patel博士によるDEFINE PCIの結果についての議論をご覧ください。
1. Davies JE, et al., DEFINE-FLAIR: A Multi- Centre, Prospective, International, Randomized, Blinded Comparison of Clinical Outcomes and Cost Efficiencies of iFR and FFR Decision-Making for Physiological Guided Coronary Revascularization. New England Journal of Medicine, epub March 18, 2017. 2. Gotberg M, et al., Instantaneous Wave-Free Ratio Versus Fractional Flow Reserve Guided Intervention (IFR-SWEDEHEART): A Multicenter, Prospective, Registry-Based Randomized Clinical Trial. New England Journal of Medicine, epub March 18, 2017. 3. Patel M. “Cost-effectiveness of instantaneous wave-Free Ratio (iFR) compared with Fractional Flow Reserve (FFR) to guide coronary revascularization decision-making.” Late-breaking Clinical Trial presentation at ACC on March 10, 2018. 4. Patel M, et al., ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients with Stable Ischemic Heart Disease. J Am Coll Cardiol. 2017 May 2;69(17):2212-2241. 5. ACC CathPCI Hospital Registry. 6. Lofti A, et al. Focused update of expert consensus statement: Use of invasive assessments of coronary physiology and structure: A position statement of the society of cardiac angiography and interventions. Catheter Cardiovasc Interv. 2018;1–12. 7. 2018 ESC/EACTS Guidelines on myocardial revascularization: The task force on myocardial revascularization of the European society of cardiology (ESC) and European association for cardio-thoracic surgery (EACTS). Eur Heart J. 2018;00:1-96. 8. An iFR cut-point of 0.89 matches best with an FFR ischemic cut-point of 0.80 with a specificity of 87.8% and sensitivity of 73.0%. (From ADVISE II, and iFR Operator’s Manual 505-0101.23. 9. Sen S, Ahmad Y, et al. Major Adverse Cardiac Events when an LAD lesion is deferred after physiological assessment by FFR or iFR: A sub-study of DEFINE FLAIR. J Am Coll Cardiol 2019. 10. Jeremias A et al. The DEFINE PCI Trial: Blinded Physiological Assessment of Residual Ischemia after Successful Angiographic Percutaneous Coronary Intervention, presented at ACC 2019.
11. Co-registration tools available within IntraSight 7 configuration via SyncVision